Thoracic Trauma - Clinical Presentation and Management - A One -Year Prospective Study in a Tertiary Care Centre in North India.
1. Abstract
1.1. Background: Thoracic injury accounts for 25 per cent of all severe injuries. Most patients who sustain thoracic trauma can be treated by technical procedures within the capabilities of clinicians trained in ATLS. This study was done to find out the incidence, causes, pattern of thoracic trauma, its diagnosis and management.
1.2.Methods: This prospective study was conducted over a period of one year on patients reporting to casualty department of IGMC, Shimla with thoracic trauma. In all patients clinical assessment was done while concomitant resuscitation was performed as per ATLS protocol.
1.3.Results: A total of 54 patients were enrolled in the study. Most common cause of injury was fall from height followed by road traffic accidents. The most common presentation was chest pain in 46 (85.2%) patients and tenderness over chest wall present in 38 (70.3%) patients. Rib fractures were present in 48 (88.8%) patients being the most common injury. Patients with associated injuries most commonly had liver injuries (25.9%). 10 (18.5%) patients were managed conservatively, 43 (79.6%) patients were managed with intercostal drainage and 1 (1.8%) patient underwent thoracotomy.
1.4.Conclusions: Thoracic trauma is a major cause of morbidity in middle aged male population. Most chest injuries are treatable with simple procedures that is tube thoracostomy and thoracotomy is rarely required. The appropriate management of these patients is rapid and accurate assessment, resuscitation, stabilisation according to priorities as per ATLS protocol followed by timely appropriate intervention and close observation/monitoring.
Keywords: Thoracic trauma; Intercostal Drainage; ICD.
Introduction
Trauma is present since the beginning of mankind. Thoracic trauma is a significant cause of mortality; in fact, many patients with thoracic trauma die after reaching the hospital. However, many of these deaths can be prevented with prompt diagnosis and treatment. Thoracic injury accounts for 25 per cent of all severe injuries. In a further 25 per cent, it may be a significant contributor to the subsequent death of the patient. Approximately, 16,000 deaths per year in India alone are a result of chest trauma. Blunt chest trauma is more common than penetrating trauma and directly comprises 20% to 25% of trauma deaths. Less than 10% of blunt chest injuries and only 15% to 30% of penetrating chest injuries require operative intervention. [1] Among patients presenting after motor vehicle collisions, higher morbidity and mortality are associated with high-speed collisions and with a lack of seat belt use. Penetrating chest trauma is associated with higher overall mortality. Incidence varies based on geographic location, predominating in urban areas, those prone to interpersonal violence, and areas of conflict.
Most patients who sustain thoracic trauma can be treated by technical procedures within the capabilities of clinicians trained in ATLS. Common life-threatening injuries are Airway obstruction, Tension pneumothorax, and Open pneumothorax, Flail chest with pulmonary contusions, Massive hemothorax and Cardiac tamponade. Potentially life threatening injuries are Simple pneumothorax, Hemothorax, Pulmonary contusion, tracheobronchial tree injury, Mild cardiac injury, Traumatic aortic disruption, Traumatic diaphragmatic injury, Blunt oesophageal rupture and Rib, sterna, scapular fractures. The physiologic consequences of thoracic trauma are hypoxia, hypercarbia, and acidosis. Contusion, hematoma, and alveolar collapse, or changes in intrathoracic pressure relationships (e.g., tension pneumothorax and open pneumothorax) cause hypoxia and lead to metabolic acidosis. Hypercarbia causes respiratory acidosis and most often follows inadequate ventilation caused by changes in intrathoracic pressure relationships and depressed level of consciousness.
Initial assessment and treatment of patients with thoracic trauma consists of the primary survey with resuscitation of vital functions, detailed secondary survey, and definitive care. Because hypoxia is the most serious consequence of chest injury, the goal of early intervention is to prevent or correct hypoxia. Injuries that are an immediate threat to life are treated as quickly and simply as possible. Most life- threatening thoracic injuries can be treated with airway control or decompression of the chest with a needle, finger, or tube. The secondary survey is influenced by the history of the injury and a high index of suspicion for specific injuries. Clinical examination can be unreliable and clinical manifestations may be delayed for hours or days. The accuracy of diagnosis increases if patient is re-evaluated repeatedly at frequent intervals.
Management of thoracic trauma is according to ALTS protocol that is primary survey, resuscitation, Secondary survey, diagnostic evaluation and definitive treatment.
This study is being done to find out the incidence, causes, and pattern of thoracic trauma, its diagnosis and management.
Methods
This prospective study was conducted over a period of one year with effect from 01/04/2020 to 31/03/2021 on patients reporting to casualty department of IGMC, Shimla with either isolated thoracic trauma or on patients of polytrauma with a component of thoracic trauma. Wherever indicated, the expert opinion of CTVS Department was sought.
Inclusion Criteria
• Patients of isolated thoracic trauma
• Patients of polytrauma with a component of thoracic trauma
• Medicolegal trauma cases were included in the study
• Patients giving a written consent and willing to participate in the study were included in the study.
Exclusion Criteria
• Patients not giving consent and not willing to participate in the study.
• Patients who were discharged against medical advice.
• The following injuries were identified and treated according to ATLS protocol
Common Life Threatening Injuries
• Airway obstruction
• Tension pneumothorax
• Open pneumothorax
• Flail chest with pulmonary contusions
• Massive hemothorax
• Cardiac tamponade
These life threatening injuries were identified and standard treatment for these life threatening injuries was initiated during primary survey followed by stabilization of the patients.
Potentially Life Threatening Injuries
• Simple pneumothorax
• Hemothorax
• Pulmonary contusion
• Tracheobronchial tree injury
• Mild cardiac injury
• Traumatic aortic disruption
• Traumatic diaphragmatic injury
• Blunt esophageal rupture
• Rib, sterna, scapular fractures
These potentially life-threatening injuries were identified and specific treatment was initiated during secondary survey.
Airway Obstruction:
Airway obstruction was managed by chin lift, jaw thrust maneuvers; oropharyngeal, nasopharyngeal, laryngeal mask, laryngeal tube airway or endotracheal intubation as the situation demanded.
Tension Pneumothorax:
Tension pneumothorax was managed initially by rapidly inserting a large caliber needle into second intercostal space in the midclavicular line of the affected hemithorax thus converting this life threatening injury into a simple pneumothorax which was then treated by inserting an underwater seal chest tube in the fifth intercostal space, just anterior to mid-axillary line.
Open Pneumothorax:
Initial management of an open pneumothorax was accompanied by promptly closing the defect with a sterile occlusive dressing large enough to overlap wound edges and then taped securely on three sides in order to provide a flutter valve mechanism. This was followed by placing a chest tube remote from the wound as soon as possible. Definite surgical closure of the defect was done later on.
Flail Chest with Pulmonary Contusion:
Initial management for patients with flail chest and pulmonary contusion was adequate analgesics, humidified oxygen and fluid resuscitation. Whenever required in some of these patients, they were put on short period of intubation and ventilation.
Massive Hemothorax:
Patients of massive hemothorax were treated by simultaneous restoration of blood volume and decompression of the chest cavity with a single (28 F) chest tube. If more than 1500 mL of blood; or one third or more of patients’ blood volume was drained in the chest tube; or if initial output of less than 1500 mL was there but patient continued to bleed, patient would require a thoracotomy. However, this decision was not be based on the rate of continuing blood loss but on the patient’s physiologic status.
Cardiac Tamponade:
The cardiac tamponade was initially managed by pericardiocentesis as it is diagnostic as well as therapeutic; though definite treatment i.e. pericardiotomy was undertaken when surgical expertise was available.
Other potentially life threatening injuries were managed as per standard protocol for their management.
Results
This study was conducted on 54 patients of thoracic trauma who presented in emergency in Indira Gandhi Medical College, Shimla from 1st April 2020 to 31st March 2021. The age of patient ranged from 8-76 years with the mean age of 42.67years. Maximum Patients i.e.15 (27.8%) belonged to the age group 41-50 followed by 31-40 i.e.12 (22.2%). 42 (77.8%) patients were males and 12 (22.2%) patients were females. Fall from height was the most common mode of injury. Of the 54 patients in our study, 32(59.2%) were injured due to fall from height, 18(33.3%) were injured in Road traffic accidents (RTA) and 2(3.7%) were injured in assault (Table 1). 51 (94.4%) patients suffered blunt trauma and 3 (5.6%) patients suffered penetrating trauma.
The most common symptom was chest pain which was complained by 46 (85.2%) patients. Shortness of breath was present in 16 (29.6%) patients. Tenderness over chest wall
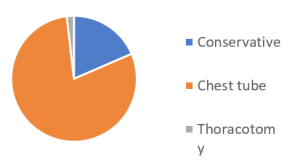
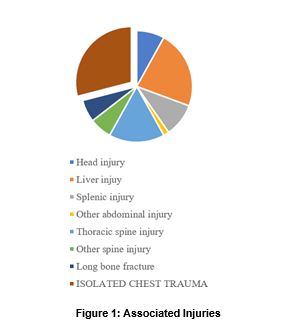
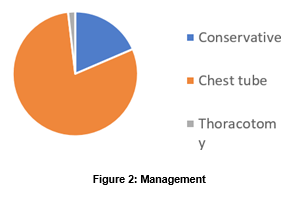
was present in 38 (70.3%) patients and was the most common sign. All the 54 patients were subjected to chest X-ray and injuries were detected in 44 (81.4 %) patients. All patients underwent eFAST which was positive for chest injury in 23 (42.6%) patients (Table 2). Among 54 patients, 4 (7.4%) had life threatening injuries. 1 (1.8%) patient had laryngeal trauma and underwent tracheostomy, 1 (1.8%) patient had tension pneumothorax and underwent urgent intercostal drainage. 2 (3.7%) patients had open pneumothorax and underwent intercostal drainage with closure of the open chest wound. 48 (88.8%) had rib fractures, 34 (63%) had hemothorax which were the most common chest injuries. Among associated injuries, liver injury was most common seen in 14 (25.9%) patients of right sided chest injuries (Figure 1). 10 (18.5%) patients were managed conservatively, 43 (79.6%) patients were managed with intercostal drainage i.e. chest tube and 1 (1.8%) patient underwent thoracotomy for penetrating chest trauma for retrieval of foreign body in the left hemithorax (Figure 2).
Discussion
In the 54 patients in our study, the age of patient ranged from 8-76 years with the mean age of 42.67years. Maximum number of patients i.e.15 (27.8%) belonged to the age group 41-50 followed by 31-40 i.e.12 (22.2%). While Sharma P et al reported the mean age at presentation of 32.8years with majority (84%) patients belonging to the age group 20-46 years [2], Sharma K et al reported that majority of the patients (31%) were from 55 to 65 years of age group (59.6±1.5) [3]. As middle-aged people are more commonly involved with outdoor activities, they are more likely to suffer trauma. Males
were affected more than females with M: F ratio of 3.5:1. Sharma P et al reported a clear male preponderance with a male to female ratio of 7:1(2). In the study by Sharma K et al it was also observed that majority of cases were male (64.2%) [3]. This dominance of the males has also been reported by various workers like Saaiq M et al, Mohan Atri et al who observed that majority (78.7%) were males. Males are more commonly injured as they are more commonly involved in activities that lead to trauma such as working at heights and driving vehicles which is a valid reason for the high male to female ratio in our study.
In our study, fall from height was the most common mode of injury (59.2). In the study by Sharma P et al, predominant mechanism of thoracic injury was road traffic accidents (RTA) in 62% patients [2]. In another study by Sharma K et al also, vehicular accident was the commonest (56.8 %) cause of injury [3]. As our hospital predominantly serves rural population of Himachal Pradesh which has a hilly terrain, fall from height seems to be the predominant mechanism of injury compared to other studies where RTA was the most common mode of injury. 51 (94.4%) patients suffered blunt trauma and 3 (5.6%) patients suffered penetrating trauma. In the area served by our hospital, assaults which most commonly cause penetrating trauma are less commonly seen. Fall from height and RTA which most commonly lead to blunt trauma form the most common causes of thoracic trauma and explain for the much higher incidence of blunt thoracic trauma compared to penetrating trauma.
The most common symptom was chest pain which was complained by 46 (85.2%) patients. In the study by Sharma K et al, chest pain was the most common (100%) presenting symptom in his study followed by breathlessness (27.2%)
[3] And results of our study are by and large comparable. On clinical examination, tachycardia was present in 12 (22.2%) patients, hypotension was present in 3 (5.6%) patients. On examination of the chest, tracheal deviation was present in 2 (3.7%) of patients, paradoxical chest movements with breathing were present in 1 (1.8%) patient, penetrating wound over chest wall was present in 3 (5.6%) patients, subcutaneous emphysema was present in 21 (38.8%) patients and tenderness over chest wall was present in 38 (70.3%) patients. On auscultation, decreased air entry on the affected side was found in 25 (46.3%) of patients and crepts were present in 4 (7.4%) patients. 8 (14.8%) patients had no signs of chest injury on clinical examination. In the study by Sharma P et al, subcutaneous emphysema was one of the presenting features in 15% cases [2] The commonest sign of presentation in the study by Sharma K et al was restricted chest movement (chest wall tenderness) due to pain (38%) followed by bony crepitation’s (29%), tachypnoea (27.2%) [3]. Kalliopi A et al stated that tachypnoea was the most common presenting feature along with localized chest tenderness [4]. Results of our study are comparable to the above studies.
All the 54 patients were subjected to chest X-ray and injuries were detected in 44 (81.4 %) patients. In the remaining 10 patients, chest X-ray showed no positive findings for chest injuries. All patients underwent eFAST which was positive for chest injury in 23 (42.6%) of patients. CT chest was done in 2 patients for chest injury and 8 patients who underwent CT for other indications (Spine and abdomen) were incidentally found to have chest injuries. These patients were found to have minor chest injuries like rib fractures or minimal hemothorax. In these patients, chest injury was not clinically apparent with no positive findings on chest X-ray.
Among patients with chest injury, 48 (88.8%) had rib fractures, 34 (63%) had hemothorax, 5 (9.2%) had
pneumothorax, 9 (16.7%) had hemopneumothorax, 1 (1.8%) had fracture sternum and 1(1.8%) had cardiac injury in the form of hemopericardium. There were no cases of mediastinal or diaphragmatic injury. In the study by Sharma P et al, 59.8% patients had haemothorax, and as many as 63% had single or multiple rib fractures [3]. Saaiq M et al found that fracture ribs were most common chest injuries (74% patients) after chest wall tenderness [5]. The findings of our study seem to be consistent with other studies.
Among all the patients, 5 (9.2%) had associated head injury, 21 (38.9%) had associated abdominal injuries and 18 (33.3%) had associated orthopaedic injuries. Among abdominal injuries, liver injury was most common seen in 14 (25.9%) patients of right sided chest injuries, splenic injury was seen in 6 (11.1%) patients with left sided chest injuries and 1 patient had ileal perforation. Among orthopaedic injuries, 10 (18.5%) patients had thoracic spine injury, 4 (7.4%) patients had spine injuries other than thoracic spine and 4 (7.4%) patients had injury to the extremities in the form of long bone fractures out of which 2 patients had fracture of the clavicle. In the study by Sharma P et al, chest injury was associated with extremity fracture in 16.85%, pelvic fracture in 8.90%, head injury in 7.15%, spinal injury in 9.85%, and maxillofacial trauma in 7.15% [2]. In the Study by Sharma K et al, majority of patients who were having chest trauma presented with associated clavicular fracture (35.2%) then followed by head injury (26.7%)[3]. In a study by Shorr et al, the most common associated injury was the abdominal trauma in 24.88% [6]. This difference in pattern of associated injuries may be explained due to different modes of injury in our study and the quoted studies.
Of all the patients of chest trauma, 10 (18.5%) patients were managed conservatively, 43 (79.6%) patients were managed with intercostal drainage i.e. under water seal chest tube and 1 (1.8%) patient underwent thoracotomy for penetrating chest trauma for retrieval of foreign body in the left hemithorax. In the study by Sharma P et al, ICD insertion was the mainstay of management in as many as 82% of the patients [2]. Most patient of chest trauma in our study were treated with conservative management as have been in the study by Sharma K et al (93.6%) [3].
Conclusion
Thoracic trauma is a major cause of morbidity in middle aged population most common in the age group of 41-50 years. Males are affected more commonly than females. Fall from height is the leading mode of injury pertaining to the hilly terrain and rural background of the study population. This can be prevented by raising awareness regarding the use of safety measures during any hazardous activity. Patients most commonly present with pain and tenderness in the injured part of chest wall with rib fractures being the most common injury. Common injuries associated with thoracic trauma are liver injuries and thoracic spine fractures. Most chest injuries are treatable with simple procedures that is tube thoracostomy and thoracotomy is rarely required. The appropriate management of these patients is adequate initial assessment and resuscitation as per ATLS protocol, timely intervention and close observation.
References
1. Advanced trauma life support, Student course manual, Tenth Edition.
2. Sharma P, Jakhmola CK. Presentation and Outcome of Thoracic Injuries at a Tertiary Care Service Hospital. Int J Sci Stud 2018; 5(10):126-130.
3. Sharma K, Tated SP, Hatkar AA. Study of the pattern and management of blunt chest injuries in rural setup. Int Surg J 2017; 4:3482-7.
4. Kalliopi A, Gerzounis M, Theakos N. Management of 150 flail chest injuries: analysis of risk factors affecting outcome. Eur J Cardio-thoracic Surg. 2004; 26:373-6.
5. Saaiq M, Shah SA. Thoracic trauma: presentation and management outcome. J Coll Physicians Surg Pak. 2008; 18(4):230-3.
6. Shorr RM, Crittenden M, Indeck M, Hartunian SL, Rodriguez A. Blunt thoracic trauma: analysis of 515 patients. Ann Surg. 1987; 206:200-5.